In 1819, the Irish doctor Samuel Black observed that angina pectoris is much less common in France than in Ireland (1). Today, after 160 years, statistics show a lower cardiovascular mortality in wine-drinking countries than in beer or spirits drinking countries (2). Then, many studies on the complex links between alcohol consumption and cardiovascular disease have created a great interest for the general public who understood the subliminal message: moderate alcohol consumption is important for preventing cardiovascular disease (3). And according to the World Health Organization, ischemic heart disease and stroke are responsible annually for about 22% of the global mortality rate (4). However, cardiovascular mortality is still low in France – despite the traditional diet including full fat cheese and delicious pastries – a phenomenon called the “French paradox”.
Some researchers have suggested that red wine is the reason of the superiority of the French’s cardiovascular health, others have contradicted them, arguing that the beneficial effect is due to ethanol from any alcoholic beverage, and others have contradicted everyone, claiming that ethanol consumed in any dose is toxic to the body. So, who’s right?
1. What does „moderate alcohol consumption“ mean?
The effects of alcohol consumption vary depending on age, gender and health status, and also on the amount consumed and on the frequency of consumption. For overall healthy people, whose age, genetics, pregnancy, illness or medication do not prohibit alcohol consumption, the definition of moderate consumption is relatively fluid.
Moderate alcohol consumption is defined by the upper limit, over which the benefits of alcohol are outweighed by the harmful effects. In agreement with this common sense definition, moderate alcohol consumption was set at:
- 1 drink per day for women
- 2 drinks per day for men.
A standard beverage contains, on average, 12-14 g of pure alcohol: 0.5 l of beer, 0.25 l of wine, or about 50 ml of brandy, vodka or whiskey (5).
– How often can we drink alcohol, under the definition of “moderate alcohol consumption”?
At the population level, moderate alcohol consumption may vary:
- from an alcoholic drink a day associated with one or both main meals (>50-100 g ethanol per week) in France,
- up to 7-14 drinks per day (> 70-140 g ethanol) in Ireland and in practically any country with people having compulsive alcohol intake only on weekends or holidays (6).
And although both patterns of consumption fall within the definition of moderate alcohol consumption, the second typology (“binge drinking” or “compulsive alcohol consumption”) is extremely dangerous, leading from acute poisoning with alcohol to alcohol coma or death (7).
– Which alcoholic drinks are healthier?
The role of wine in explaining the French paradox is questionable because, statistically, the beneficial effects of active substances in wine arise from a high wine consumption (8).
Some studies suggest that red wine is beneficial (9).
Other studies – that wine of any color and beer offer cardiovascular benefits superior to spirits drinks(10).
And other studies suggest that ethanol in any alcoholic drink produces the same cardiovascular effects (11).
2. What are the positive effects of moderate alcohol consumption?
Apparently, the hypothesis that moderate alcohol consumption prevents cardiovascular disease and decreases the incidence of mortality from this cause seems to make sense. Epidemiological evidence suggests a J-shaped relationship (Figure 1) between alcohol consumption and mortality (12).
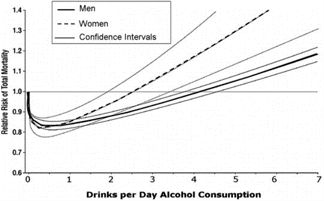
Figure 1. DiCastelnuovo et al. Alcohol dosing and total mortality, 2006.
The mechanisms behind the protective effects could be:
- increasing the blood level of high density lipoproteins cholesterol (HDL-c),
- lowering the blood level of low density lipoproteins cholesterol (LDL-c),
- preventing the blood clots formation by reducing platelet aggregation.
Thus, moderate alcohol consumption might reduce cardiovascular risk, both by inhibiting atheromatosis, and by lowering the blood coagulation rate.
– Does moderate alcohol consumption increase HDL-cholesterol?
An HDL-c blood level below 40 mg/dl is associated with an increased risk of cardiovascular disease, even in people whose total cholesterol and LDL-c blood levels are within the normal range (13).
HDL-c between 40 and 60 mg/dl is considered “neutral” and does not affect cardiovascular risk.
And HDL-c above 60 mg/dl is associated with a reduced cardiovascular risk – representing the goal for prophylaxis of the cardiovascular disease.
We can increase HDL-c by:
- quitting smoking,
- decreasing the percentage of body fat
- through regular sports, and
- through a diet based on:
- increased fiber, omega-3 fatty acids and antioxidants intake
- reducing or eliminating trans fats (14).
Studies suggest that moderate alcohol consumption reduces the risk of atherosclerosis and the main mechanism seems to be the ability to increase HDL-c concentration (15). However, the mechanisms by which alcohol determines thisHDL-c increase are not fully understood.
Some researchers have suggested that alcohol increases HDL cholesterol by increasing the transport rate of apolipoproteins A-I and A-II (16). Others have explained the effect by stimulating cells’ cholesterol efflux and its esterification in plasma (17).
However, regardless of the mechanism by which moderate alcohol consumption increases HDL-c, moderate alcohol consumption still contributes to an increased triglycerides blood level (18). And the increase of the triglycerides blood level is an independent risk factor for cardiovascular disease (19).
– Does moderate alcohol consumption lower LDL-cholesterol?
The effects of moderate alcohol consumption on blood levels of LDL-c are unclear.
From studies that found only a small LDL-c lowering effect of only 0.1 mmol/l, following a daily consumption of 15-30 g of alcohol per day for 8 weeks (20), to studies that found a hypolipidemic effect in young people only, and the opposite effect, of increasing LDL-c, in elderly adults (21), to studies that found LDL-c decreases only for moderate daily alcohol consumption, and the opposite effect, of increasing LDL-c, for moderate but compulsive consumption (22) – the many conclusions of scientists are very contradictory, sounding more like assumptions and biased personal opinions than science.
On the other hand, a 2003 study showed that dealcoholised wine has an LDL-c lowering effect similar to atorvastatin (Lipitor), 20% higher than that of natural alcohol – suggesting that ethanol in wine actually masks the hypolipidemic effect of polyphenols (23).
So we’re back to the question: is the alcohol or the polyphenol within a Mediterranean diet the basis for the famous French paradox?
– Does moderate alcohol consumption have antithrombotic effects?
In addition to influencing the LDL-c / HDL-c ratio, moderate alcohol consumption affects coagulation factors (fibrinogen, coagulation factor VII and von Willebrand factor), thus having antithrombotic effects (24).
However, Rantakömi et al. showed that overweight and hypertensive patients with moderate alcohol consumption have an increased risk of ischemic stroke compared to those who don’t drink (25).
The obesity epidemic should therefore be counted in before recommending moderate alcohol consumption as a means of cardiovascular prevention.
Also, compulsive alcohol consumption is associated with inhibition of fibrinolysis, which contributes to the unstable balance between moderate alcohol consumption and cardiovascular mortality (26).
3. What are the negative effects of moderate alcohol consumption?
Any benefits of moderate alcohol consumption on mortality are abolished at an excessive consumption level by increasing the risk of death due to:
- alcoholic cardiopathy,
- paroxysmal tachycardia,
- depression,
- cancer,
- cirrhosis,
- traffic accidents.
– Does moderate alcohol consumption have arrhythmic effects?
Atrial fibrillation (AF) is the most common cardiac arrhythmia, and the close relationship between compulsive alcohol and AF (even in healthy people) has been known for decades. Of course, the causal relationship is directly proportional to the dose, but the amount of alcohol needed to increase the risk of AF is only of 2 alcoholic drinks a day for women and 4 for men (27).
So, simply doubling the amount of 1 drink per day in women and 2 in men increases the risk of atrial fibrillation.
Also, regular alcohol intake has cumulative effects, potentially affecting left ventricular function of the heart long before cardiac abnormalities become symptomatic.
Thus, moderate alcohol consumption depresses cardiovascular function, the deterioration progressing:
- from the isolated impairment of the heart muscle pump function
- to cardiomegaly and, finally,
- to decompensation (28).
– Does moderate alcohol consumption have hepatotoxic effects?
Paradoxically, the hepatic effects of moderate alcohol consumption are even more controversial than cardiac effects.
On one hand, some studies show a beneficial effect of moderate alcohol consumption, associating a low incidence of liver steatosis:
- both in healthy people (29),
- as well as in people with high cardiac risk (30).
On the other hand, the so-called hepatic alcohol benefits are considered by many clinicians purely epidemiological (31).
Also, a study of 18,899 people aged 25 to 74 demonstrated that:
- men over the age of 40 who consumed over 8 alcoholic drinks per week – but remained within the moderate 7-14 permitted drinking range for males – had elevated liver transaminases, despite the lack of any symptoms;
- in men under 40, the effect occurs at a consumption of 14 alcoholic beverages per week (32).
– Does moderate alcohol consumption have carcinogenic effects?
Studies show an obvious causal link between excessive alcohol and cancer (33).
However, it seems that also moderate alcohol consumption can be carcinogenic (34).
Different factors may contribute to the pathogenesis of cancer associated with moderate alcohol consumption, including the actions of acetaldehyde, the most toxic metabolite of alcohol. Acetaldehyde itself is carcinogenic, being used to generate cancer in laboratory animals. In addition, highly reactive molecules that are generated during alcohol metabolism can damage DNA, thus increasing the carcinogenic potential of acetaldehyde (35).
Moderate alcohol consumption is responsible for the increased risk of digestive tract cancers (36). And, in addition to the carcinogenic potential, regardless of the type and dose of alcohol consumed, alcohol facilitates the occurrence of gastroesophageal reflux disease by reducing lower esophageal sphincter pressure and esophageal motility.
Another type of cancer strongly associated epidemiologically with moderate alcohol consumption is breast cancer, both in women and men – a fact ignored by the recommendation that moderate alcohol consumption is part of a healthy lifestyle (37).
4. What are the bias factors in studies researching the effects of moderate alcohol consumption?
Many studies on the effects of moderate alcohol consumption have produced highly contradictory results (38).
– What are the bias factors responsible for these contradictory results?
Some of the causes of these contradictory results may be the design of the study and the hidden variables, sometimes more significant in inducing the epidemiological results than the presumed causal variables of the study.
An objective study on the effects of ethanol should be:
- controlled randomized – subjects shared randomly as non-alcohol users, moderate consumers, compulsive and alcoholic consumers, with no difference between groups other than the variables to be studied,
- double-blind – neither subjects nor researchers will know who receives alcohol and who receives placebo,
- longitudinal – to study the same subjects over time
- performed on a sufficiently long term – subjects should not change the pattern of alcohol consumption throughout the study to continue to be part of the group they were originally classified in.
The cost and logistics of such a study are the reasons cited in support of the fact that these studies are based on individual (often retrospective) reports and on the subjective definitions of groups of participants – methods that do not guarantee the accuracy of the data collected (39).
The definition of abstainers (non-alcohol users) in many studies refers only to people who did not consume alcohol in the last month (40).
Thus, it is not surprising that the group of moderate alcohol consumers is healthier than the group of abstainers – if we introduce them under the generic name of “abstainers”:
- former alcoholics – with an increased risk of ischemic cardiopathy, hypertension, diabetes, ulcer, biliary dyskinesia and bronchitis
- sick people – whose illness or medication prevented them from consuming alcohol in the month prior their enrolling in the study.
The bad health condition of many people in the group of abstainers should not be evidence of the benefits of drinking (41).
However, even in studies in which abstinence includes people who have not consumed alcohol for one year, the inclusion of former alcoholics is tendentious, because former alcoholics have a cardiovascular risk of up to twice as high.
The association between moderate alcohol consumption and cardiac protection disappears after the former alcoholics are removed from the group of abstainers (42).
It is true that an alcoholic beverage can increase the mood and palatability of the foods consumed at the meal, but the real problem is that very few people consume alcohol in moderation – most either completely avoids alcohol for days and then consumes too much once or consumes more than moderate each time (43).
Attempting to promote moderate alcohol consumption among abstainers and to somehow excuse it among more or less moderate consumers is healthy for the alcohol industry.
But for people, the benefits more fluid.
Quoted studies
1. Black S. Clinical and Pathological Reports. Newry, UK: Alex Wilkinson, 1819, p. 1–47.
2. St. Leger AS, Cochrane AL, Moore F. Factors associated with cardiac mortality in developed countries with particular reference to the consumption of wine. Lancet 1: 1018–1020, 1979.
3. Casswell S. Public discourse on the benefits of moderation: implications for alcohol policy development. Addiction, 88(4), 459-465, 1993.
4. The top 10 causes of death. (Updated July 2013) http://www.who.int/mediacentre/factsheets/fs310/en/index.html
5. National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much: A clinician’s guide (updated) Washington, DC: National Institutes of Health; 2007. NIH Publication No. 07-3769.
6. Ruidavets, Jean-Bernard et al. Patterns of alcohol consumption and ischaemic heart disease in culturally divergent countries: The Prospective Epidemiological Study of Myocardial Infarction (PRIME). BMJ: British Medical Journal 341 (2010). doi: http://dx.doi.org/10.1136/bmj.c6077
7. 3.1.3. Mukamal K.J., Conigrave K.M., Mittleman M.A., Camargo CA. Jr., Stampfer M.J., Willett W.C., Rimm E.B. Roles of drinking pattern and type of alcohol consumed in coronary heart disease in men. N Engl J Med 348: 109–118, 2003.
8. Holahan, C. J., Schutte, K. K., Brennan, P. L., North, R. J., Holahan, C. K., Moos, B. S., & Moos, R. H. (2012). Wine consumption and 20-year mortality among late-life moderate drinkers. Journal of studies on alcohol and drugs,73(1), 80.
9. Streppel M. T., Ocké M. C., Boshuizen H. C., Kok F. J., & Kromhout D. (2009). Long-term wine consumption is related to cardiovascular mortality and life expectancy independently of moderate alcohol intake: the Zutphen Study. Journal of epidemiology and community health, 63(7), 534-540. doi:10.1136/jech.2008.082198.
10. Costanzo S., Di Castelnuovo A., Donati M. B., Iacoviello L., & de Gaetano G. (2011). Wine, beer or spirit drinking in relation to fatal and non-fatal cardiovascular events: A meta-analysis. European journal of epidemiology, 26(11), 833-850.
11. Krnic M., Modun D., Budimir D., Gunjaca G., Jajic I., Vukovic J., … & Boban M. (2011). Comparison of acute effects of red wine, beer and vodka against hyperoxia-induced oxidative stress and increase in arterial stiffness in healthy humans. Atherosclerosis, 218(2), 530-535. http://dx.doi.org/10.1016/j.atherosclerosis.2011.07.004
12. DiCastelnuovo A., Castanzo S., Bagnardi V., Donati M.B., Iacoviello L., de Gaetano G. Alcohol dosing and total mortality in men and women. Arch Intern Med. 166 2006:2437-2445.
13. Cui Y., Blumenthal R. S., Flaws J. A., Whiteman M. K., Langenberg P., Bachorik P. S., & Bush T. L. (2001). Non-high-density lipoprotein cholesterol level as a predictor of cardiovascular disease mortality. Archives of Internal Medicine, 161(11), 1413. doi:10.1001/archinte.161.11.1413.
14. O’Donnell Martin J., et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): A case-control study. The Lancet 376.9735 (2010): 112-123.
15. Boden, William E. High-density lipoprotein cholesterol as an independent risk factor in cardiovascular disease: Assessing the data from Framingham to the Veterans Affairs High-Density Lipoprotein Intervention Trial. The American journal of cardiology,
86.12 (2000): 19-22.
16. De Oliveira et al. Alcohol consumption raises HDL cholesterol levels by increasing the transport rate of apolipoproteins AI and A-II. Circulation 102.19 (2000): 2347-2352. doi: 10.1161/01.CIR.102.19.2347
17. Van der Gaag M. S., Van Tol A., Vermunt S. H. F., Scheek L. M., Schaafsma G., & Hendriks H. F. J. (2001). Alcohol consumption stimulates early steps in reverse cholesterol transport. Journal of lipid research, 42(12), 2077-2083.
18. Van de Wiel, Albert. The effect of alcohol on postprandial and fasting triglycerides. International journal of vascular medicine 2012 (2011).
19. Nordestgaard B. G., Benn M., Schnohr P., & Tybjærg-Hansen A. (2007). Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA: the journal of the American Medical Association, 298(3), 299-308.
20. Baer, David J. et al. Moderate alcohol consumption lowers risk factors for cardiovascular disease in postmenopausal women fed a controlled diet. The American journal of clinical nutrition 75.3 (2002): 593-599.
21. Whitfield J. B., Heath A. C., Madden P. A., Pergadia M. L., Montgomery G. W., & Martin N. G. (2012). Metabolic and Biochemical Effects of Low‐to‐Moderate Alcohol Consumption. Alcoholism: Clinical and Experimental Research. doi: 10.1111/acer.12015
22. Liu W., Redmond E. M., Morrow D., & Cullen J. P. (2011). Differential effects of daily-moderate versus weekend-binge alcohol consumption on atherosclerotic plaque development in mice. Atherosclerosis, 219(2), 448-454.
23. Pal, S., Ho, N., Santos, C., Dubois, P., Mamo, J., Croft, K., & Allister, E. (2003). Red wine polyphenolics increase LDL receptor expression and activity and suppress the secretion of ApoB100 from human HepG2 cells. The Journal of nutrition, 133(3), 700-706.
24. Lacoste, Lucie, Joseph Hung, and Jules YT Lam. Acute and delayed antithrombotic effects of alcohol in humans. The American journal of cardiology 87.1 (2001): 82-85.
25. Rantakömi, Sanna H. et al. Alcohol consumption and the risk of stroke among hypertensive and overweight men. Journal of neurology 260.2 (2013): 534-539.
26. Kiviniemi Tuomas O. et al. High dose of red wine elicits enhanced inhibition of fibrinolysis. European Journal of Cardiovascular Prevention & Rehabilitation 16.2 (2009): 161-163.
27. Zimmermann, A. J., & Conen, D. (2012). How Does Alcohol Intake Relate to the Risk of Atrial Fibrillation?. JAFIB: Journal of Atrial Fibrillation, 5(4).
28. Ahmed, S. Sultan, and Timothy J. Regan. Heart muscle diseases. The Cardiomyopathies Part III. Cardiotoxicity of alcoholism. Pakistan Heart Journal 14.3 (2012).
29. Gunji Toshiaki et al. Light and moderate alcohol consumption significantly reduces the prevalence of fatty liver in the Japanese male population. The American Journal of Gastroenterology 104.9 (2009): 2189-2195.
30. Dunn, Winston, Ronghui Xu, and Jeffrey B. Schwimmer. Modest wine drinking and decreased prevalence of suspected nonalcoholic fatty liver disease. Hepatology 47.6 (2008): 1947-1954.
31. Liangpunsakul Suthat, and Naga Chalasani. What Should We Recommend to Our Patients with NAFLD Regarding Alcohol. The American journal of gastroenterology 107.7 (2012): 976-978.
32. Tynjälä Joanna et al. Effect of age and gender on the relationship between alcohol consumption and serum GGT: time to recalibrate goals for normal ranges. Alcohol and alcoholism 47.5 (2012): 558-562.
33. Nelson, David E. et al. Alcohol-attributable cancer deaths and years of potential life lost in the United States. American journal of public health 103.4 (2013): 641-648.
34. Bagnardi V. et al. Light alcohol drinking and cancer: A meta-analysis. Annals of oncology 24.2 (2013): 301-308.
35. Boffetta Paolo, and Mia Hashibe. Alcohol and cancer. The lancet oncology 7.2 (2006): 149-156.
36. Laffoy, M. et al. Cancer Incidence and Mortality due to Alcohol: An Analysis of 10-Year Data. Irish (2013): 294.
37. Guénel, Pascal et al. Alcohol drinking may increase risk of breast cancer in men: A European population-based case-control study. Cancer Causes & Control 15.6 (2004): 571-580.
38. Roerecke Michael, and Jürgen Rehm. The cardioprotective association of average alcohol consumption and ischaemic heart disease: A systematic review and meta‐analysis. Addiction 107.7 (2012): 1246-1260. doi: 10.1111/j.1360-0443.2012.03780.x
39. Babor Thomas F. et al. Talk is cheap: measuring drinking outcomes in clinical trials. Journal of Studies on Alcohol and Drugs 61.1 (2000): 55.
40. Di Castelnuovo A., Costanzo S., Bagnardi V., Donati M.B., Iacoviello L., de Gaetano G. Alcohol dosing and total mortality in men and women: An updated meta-analysis of 34 prospective studies. Archives of Internal Medicine. 2006;166: 2437–2445.
41. Fillmore K. M., Kerr W. C., Stockwell T., Chikritzhs T., & Bostrom A. (2006). Moderate alcohol use and reduced mortality risk: Systematic error in prospective studies. Addiction Research & Theory, 14(2), pag. 101-132. doi:10.1080/16066350500497983.
42. Kloner Robert A., and Shereif H. Rezkalla. To drink or not to drink? That is the question. Circulation, 116.11(2007):1306-1317. doi:10.1161/CIRCULATIONAHA.106.678375.
43. Ruidavets Jean-Bernard et al. Patterns of alcohol consumption and ischaemic heart disease in culturally divergent countries: the Prospective Epidemiological Study of Myocardial Infarction (PRIME). BMJ: British Medical Journal 341 (2010).