The story of the virus with a beer name (Coronavirus, so: Have it with lime!) began at a market.
On December 30, 2019, in a small fish and meat market where 1500 worked, in a crowded Chinese city with 11 million inhabitants, some workers got sick. And because they felt quite sick, each decided to go see a doctor in the hope that they still could somehow spend the New Year’s Eve in the family. And this is how the Wuhan on-call doctors got to see these patients suffering from a type of pneumonia that was not very responsive to traditional treatments. (1)
They scratched their heads for days and nights and tried their best to deal with the weird flu until – January 7, 2020 – when dr. Shi Zhengli’s team, a local virologist, informed them that the strange disease is a zoonosis caused by a virus from the Coronavirus family which normally affects bats.
We do not know if the pandemic declared on Wednesday by the World Health Organisation (WHO) broke out because the use of soap is one of the behaviours that distinguish people from animals or because some people have started to eat vampire bats. However, as direct descendants of father Dracula, we should take the stories of humans eating vampires at least with a grain of salty garlic.
Because the panic and the brain work in shifts, Coronavirus managed to divide the planet in two:
- either you are scared – and you just realised that soap was invented
- either you are rational – and you look in dismay at how seemingly mentally healthy people started to queue up to buy soap
Well… there is also the third category: the careless people continuing to live their lives like nothing happens on the planet.
This article is not a call to carelessness, it is a call to reason.
Because panic amplifies irrational behaviours whose consequences can unbalance us all, it is important to see the situation as it is: neither better, nor worse than it is.
The problem is complicated not only by the fact that fear freezes the brain, but also by the fact that the very brain humans operate on comes with at least one factory defect:
The more we read and hear about a thing that rarely happens the more we expect it to happen despite knowing deep in our minds that it rarely happens – which is called “availability bias“. (2)
The more we hear about Coronavirus, the more it looks like it sits and looks at us through the kitchen window like a vampire – ready to jump and grab us by the shoulders to suck out our lungs.
Researchers warned us for years and years that the way pandemic infectious diseases are communicated and managed has a major financial impact, the perception of risk having a more harmful impact than the disease itself. (3)
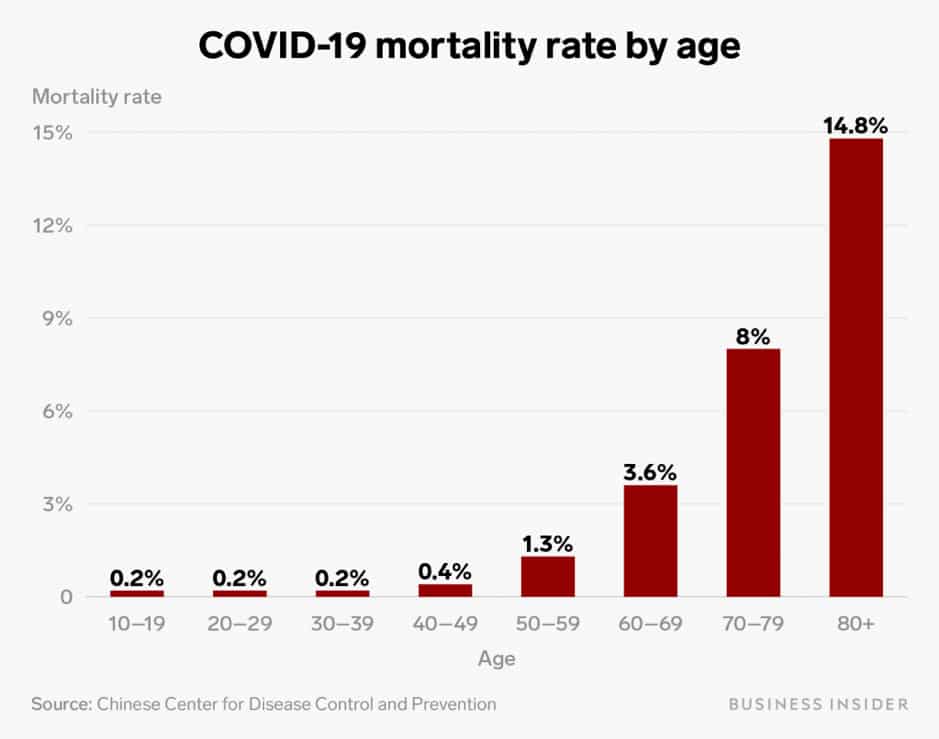
In the rare times when we would still decide to use our neocortex, we could look at Chinese officials report which shows that:
- 81% of infected people had only mild respiratory symptoms if at all, more than half presenting without having a fever
- 14% of infected people developed severe respiratory disease, needing Intensive Care
- and the 5% of the infected people that developed severe respiratory disease who put their lives at risk were sick and old, most very sick and very old (4)
Despite official reports showing that most people who get infected only develop mild respiratory disease, on Wednesday – March 11, 2020, WHO declared the current global situation a pandemic because the number of cases reached 118,000 worldwide, of which 4,291 have died.
Risk perception doubled since pandemic has been declared in spite of the fact that even in Italy – the most affected country besides China – official reports show that 91% of infected people have only mild disease.
The majority of people do not understand what a pandemic actually means, although the flu regularly reaches pandemic levels and although most – even those very ill or exposed – usually ignore it and refuse to get vaccinated.
But what we know from the former pandemics we went through is that the most harmful impact is generated by people’s perception of risk, affecting mainly the economy of the countries not the health of the people.
Pandemic does not mean that the disease has changed or that it became more aggressive.
Pandemic means that many people are affected worldwide.
It shows the disease is highly contagious, not highly aggressive.
– How many of us haven’t had a cough or a fever this winter?
According to the report published by WHO on March 12, Coronavirus mortality is 3.6% – a simplistic figure obtained by dividing the number of deaths by the number of officially known cases.
And this simplistic figure built on the known cases is the root of all mathematical speculations that feed people’s panic. But it’s a fake number.
Although the 3.6% mortality rate looks enormous when compared to the minuscule 0.1% mortality rate of the flu, most experts remain quite calm stating that if you compare apples with pears lice come out when the aliens no longer land in Antarctica because Tuesday is blue.
Most infectious disease experts remain calm because of the 118.000 people officially infected with Coronavirus those who got severely affected were either very old or already very sick before catching up the virus, having multiple other diseases besides the last drop of corona.
And most mathematics experts remain calm because without proper testing the powerful stage effect – obtained by the fervent media coverage of the shiny 3.6% COVID-19 mortality as “huge” when compared with the 0.1% flu mortality – cannot wipe out the only two things we actually know despite the global madness:
- of 100 people infected with Coronavirus 96,4 survive
- the 3.6% mortality figure is a fake number because it is based on the number of officially known cases not on the actual number of cases
Just that not all mathematicians remain calm, some mathematicians making statistical estimates based – maybe – on accepting the fact that in general the masses of panicked people behave irrationally, and individually many people do not care enough about other people to respect minimum common sense recommendations.
It seems that common sense is not that common.
Besides the low incidence of common sense, the mathematicians who don’t remain calm quote the exponential growth bias – another bias that usually affects human’s thinking. According to this thinking flaw, most people do not understand that a small problem can grow exponentially, so they ignore it. (5)
But the mathematicians that remain calm in this global madness state that Coronavirus pandemics doesn’t present exponential growth and that the prediction models built on exponential growth mathematical models can be misused in pandemics. (6)
Because of insufficient testing:
- and, because the majority of infected people don’t even have a fever, we cannot know that the known number of cases is the number of cases
- and, because the mortality figure is obtained by dividing the number of deaths to the number of known cases, the mortality figure would be very different if we would know the actual number of cases
- and, because of the induced panic, the mathematically built worldwide problem will end up costing us all financially as the economy will take the actual fall (7)
Based on the fact that current statistics confirm the initial Chinese report proving that more than 80% of the people who get infected with Coronavirus have no or only mild symptoms – purely mathematically – the total number of worldwide cases could be 5 times higher than the officially known number.
And this would mean nothing bad if we’d had the discipline and the responsibility to respect the minimum recommended prevention.
A higher number of cases does not mean that the disease is more aggressive.
A higher number of cases means the disease is more contagious.
More contagious does not mean more aggressive.
Aggressivity is about the probability of dying from the disease not about just getting the disease.
COVID-19 is contagious. SARS was aggressive.
Theoretically, we are required to do the least possible: to stay in the house when we have respiratory symptoms or when we know that we’ve just traveled back from areas affected by the virus, not to kiss the elderly and to wash our hands. But for common sense recommendations to be effective you have to have common sense. And because many do not have common sense, prolonging the application of these initially minimum recommendations, cumulatively will end up highly expensive for all.
Each pandemic is different depending on:
- disease factors: how contagious it is and how aggressive it is
- human factors: like the age and state of health or hygiene
- health system factors: such as adequate access to protective equipment, the capacity of intensive care units and the fact that physicians and other unprotected medical personnel can become the first line of victims of others’ panic and lack of common sense
- science factors: how fast researchers can come up with:
- diagnostic kits able to accurately identify affected individuals
- effective treatments for the current outbreak
- vaccines to prevent future ones
If the disease induced by the Coronavirus infection is more contagious but 80% of the infected people just cough, most without even having a fever, then the global number of cases could be 590.000, and mortality 0.7%.
And yes, 0.7 is still 7 times higher than the 0.1 flu mortality, but this does not erase the fact that from 100 Coronavirus-infected people 99.3 will be ok.
But you cannot say anymore that 99.3 of 100 infected people will be ok after the economic consequences of the assumptions you officially trumpeted began to emerge, exactly as you patchily did in 2003 with the far more aggressive SARS. (8)
Aligned with the many thinking biases described by Tversky and Kahneman in the 1970s, once they take an official stance most people tend to continue to defend it even when their own evidence contradicts them. And those managing the COVID-19 pandemic are people too. So the global madness will continue based on the only factor they can pin down: the high contagiousnessț impact on the exponential growth.
But the evolution of the disease does not show exponential growth.
When the reality of the disease contradicts you but the economic consequences of the wrong statistic presumptions you made have begun to appear, you cling to any evidence that might justify what you assumed:
- the population at higher risk
- and the fall of the medical system
To protect yourself from the economic consequences of the panic created globally, of the 100 infected that mostly have nothing you fervently put the spot light on the only 1 that’s doing worse and hope that no one with sufficient economic and political power will grab you by the collar to ask why the hell do you put the spot light on this 1 when 99.3 are fine.
Just that treating the population at higher risk and the resources required for the medical system to keep working cost money and all systems risk to fall including the medical system when there will be no money because we neglected economy while trying to preserve health.
The disease induced by Coronavirus is mainly mild.
Without proper testing, mortality seems higher than influenza’s but officially available mortality figures don’t indicate an exponential growth.
People that were already damaged by advance age or advanced disease before Coronavirus will be more affected.
Health care systems that were already damaged before the Coronavirus will be more affected.
Officially, WHO recommends:
- to greet each other at least one meter distance
- to cough in the elbow
- to stay home if we feel ill
- to wash our hands
- and to clean up our homes and spaces
Officially, WHO doesn’t even recommend to wear a mask without first having cough or a fever, specialists recommending them only to those having symptoms and to those taking care of them because:
- most masks available on the market are not appropriate
- most people who have access to appropriate masks do not use them properly
- and because the actual number of masks and other protective medical devices available on the planet is limited, even the medical personnel risking to remain without them due to the panic created in the general population
However, in spite of the fact that unlike the flu Coronavirus doesn’t seem to severely affect children and teenagers and in spite of the available analyses of past pandemics showing that school closure has tripled economic harm in countries such as England, France, Belgium and the Netherlands (9), the UNICEF and WHO stands is the quoted reason behind the closure of schools.
– Who cares that school closure and the absenteeism generated by panic worsens the economic impact? (10)
Ignoring the fact that everyone’s access to any medical treatment decreases if our financial capacity drops down to caves levels, we close schools to protect the 3.6 grandparents out of those 100 grandparents over the age of 80 or with more illnesses than they can carry assuming they might get infected by their grandchildren who’d go to school.
And while schools are deserted to protect the vulnerable grandparents, the parks are full with vulnerable grandparents taking their grandchildren out to have some fun like in a global unplanned holiday.
The disease is mild and the spread might end if 76% of transmissions would stop. (11) But adding to the fact that the vulnerable population seems to mock our efforts to protect them, some of the people officially diagnosed as being infected with Coronavirus do not respect the fact that by leaving the house others will be infected.
Just like for years, as a mother, I had to deal with the consequences of other parents bringing their sick children to school despite the risk of infecting other children – of a mild flu – now we witness in dismay how people at risk and people officially infected or people who traveled back from high risk areas of the globe just casually go outside, enjoying the spring warm weather.
We respectfully stay home to protect the vulnerable population, while the vulnerable population casually goes out to the beach, having barbecues, meeting their friends at the mall then panically buying everything that falls into their hands, sitting at endless queues for food and soap.
We stay home although we could work.
Old people and those diagnosed with or at risk of a coronavirus infection are walking the streets spending their last dime on beans, vitamins and soap resting assured that the Easter Bunny and Santa Claus will take care of them when they will eventually run out of money.
– What are you going to eat a month from now if you spend all your money today on perishables?
– Face masks and soap?
Reading official reports, during the past few weeks I wondered if we globally went batshit crazy …
Not that I complain of the light traffic in Bucharest or of the joy of my children generated by the unplanned holiday that gradually translated to boredom. But Coronavirus has filled my Inbox with two types of emails:
- some making the same demand: “What should I buy to increase my immunity?“
- and some making the same offer: “What can we sell you to increase your immunity?“
Like at the market: demand and supply.
And if the answer to the second question is a simple SPAM report thinking “the mother of the idiots is always pregnant“, the answer to the first question seems somewhat more complicated because the vast majority of people think this is THE time when you have to take something to increase your damn immunity.
Obviously, the vast majority of people does not want to address the fact that eating fast food and drinking soda drinks on the run (12) during stressful days followed by nights with low quality, insufficient sleep (13) decreases immunity.
The vast majority of people has no idea what “immunity” is, the subliminal message passed on from one good doer to another being that you have to take vitamins, antioxidants or something.
Most believe that “immunity” is bought at the pharmacy.
Just that only “immunity” is bought at the pharmacy.
Immunity without quotation marks depends on the healthy eating (14), on the regular life-long practice of sports (15, 16), on the high quality sleep (17), and even on the well-being and overall happiness level of your life (18). So yes, it seems damn tricky to increase immunity so suddenly now with this Coronavirus sneaked out of the dark Chinese vampires’ caves in the fast food-sedentary-stressful-unhappy life.
Just that, although we are encouraged to take all sorts of stuff to somehow defend ourselves against this dark virus, the only two things you can actually do to increase your immunity specifically against Coronavirus are:
- to get infected with Coronavirus
- to get vaccinated with a vaccine specifically created against this virus
We have no vaccine yet.
And exactly as everybody wants to go to heaven, but nobody wants to die, there isn’t anybody who’d want to get infected.
Without getting sick and without the vaccine, the only thing you can increase by taking all sorts of vitamins, plants and miracle natural remedies is is the non-specific part of the immune system, the innate immunity.
But increased non-specific immunity does not specifically defend you against Coronavirus or against anything else for that matter.
Non-specific immunity is called “non-specific” because it is non-specific.
And increasing non-specific immunity does not mean improved health.
Increased non-specific immunity means deregulated immune system, bone and gastrointestinal inflammatory disease, allergies, autoimmunity. (19)
And it is absolutely pointless to take any magic plant or vitamin for the purpose of increasing non-specific immunity.
Non-specific immunity is directly increased by stress, sedentariness, insufficient sleep and by the very western diet by their pro-inflammatory effects. (20)
Immunity without quotation marks is a much more complex system than it seems when talking about immunity while having a Corona.
The upside of the Coronavirus story is that it has managed to increase interest in seemingly uninteresting products. Like soap.
The downside is that if this global panic continues, we will not die of Coronavirus but of poverty.
It all started at the market and it will all end at the market.
I’m not sure if it’s like at the small fish and meat market in Wuhan where some of the 1500 workers got infected, but all this seems kind of an expensive trade that ignores the fact that in order to have something to sell someone still has to actually work.
References
(13) Prather, Aric A. “Sleep, stress, and immunity.” Sleep and Health. Academic Press, 2019. 319-330.
(17) Ganz, Freda DeKeyser. “Sleep and immune function.” Critical care nurse 32.2 (2012): e19-e25.



